A nervous system that functions correctly is a fantastically complex, well-oiled machine—synapses fire appropriately, muscles move when needed, memories are formed and stored, and emotions are well regulated. Unfortunately, each year millions of people in the United States deal with some sort of nervous system disorder. While scientists have discovered potential causes of many of these diseases, and viable treatments for some, ongoing research seeks to find ways to better prevent and treat all of these disorders.
Neurodegenerative Disorders
Neurodegenerative disorders are illnesses characterized by a loss of nervous system functioning that are usually caused by neuronal death. These diseases generally worsen over time as more and more neurons die. The symptoms of a particular neurodegenerative disease are related to where in the nervous system the death of neurons occurs. Spinocerebellar ataxia, for example, leads to neuronal death in the cerebellum. The death of these neurons causes problems in balance and walking. Neurodegenerative disorders include Huntington’s disease, amyotrophic lateral sclerosis, Alzheimer’s disease and other types of dementia disorders, and Parkinson’s disease. Here, Alzheimer’s and Parkinson’s disease will be discussed in more depth.
Alzheimer’s Disease
Alzheimer’s disease is the most common cause of dementia in the elderly. In 2012, an estimated 5.4 million Americans suffered from Alzheimer’s disease, and payments for their care are estimated at $200 billion. Roughly one in every eight people age 65 or older has the disease. Due to the aging of the baby-boomer generation, there are projected to be as many as 13 million Alzheimer’s patients in the United States in the year 2050.
Symptoms of Alzheimer’s disease include disruptive memory loss, confusion about time or place, difficulty planning or executing tasks, poor judgment, and personality changes. Problems smelling certain scents can also be indicative of Alzheimer’s disease and may serve as an early warning sign. Many of these symptoms are also common in people who are aging normally, so it is the severity and longevity of the symptoms that determine whether a person is suffering from Alzheimer’s.
Alzheimer’s disease was named for Alois Alzheimer, a German psychiatrist who published a report in 1911 about a woman who showed severe dementia symptoms. Along with his colleagues, he examined the woman’s brain following her death and reported the presence of abnormal clumps, which are now called amyloid plaques, along with tangled brain fibers called neurofibrillary tangles. Amyloid plaques, neurofibrillary tangles, and an overall shrinking of brain volume are commonly seen in the brains of Alzheimer’s patients. Loss of neurons in the hippocampus is especially severe in advanced Alzheimer’s patients. Figure 16.30 compares a normal brain to the brain of an Alzheimer’s patient. Many research groups are examining the causes of these hallmarks of the disease.
One form of the disease is usually caused by mutations in one of three known genes. This rare form of early onset Alzheimer’s disease affects fewer than five percent of patients with the disease and causes dementia beginning between the ages of 30 and 60. The more prevalent, late-onset form of the disease likely also has a genetic component. One particular gene, apolipoprotein E (APOE) has a variant (E4) that increases a carrier’s likelihood of getting the disease. Many other genes have been identified that might be involved in the pathology.
Unfortunately, there is no cure for Alzheimer’s disease. Current treatments focus on managing the symptoms of the disease. Because decrease in the activity of cholinergic neurons (neurons that use the neurotransmitter acetylcholine) is common in Alzheimer’s disease, several drugs used to treat the disease work by increasing acetylcholine neurotransmission, often by inhibiting the enzyme that breaks down acetylcholine in the synaptic cleft. Other clinical interventions focus on behavioral therapies like psychotherapy, sensory therapy, and cognitive exercises. Since Alzheimer’s disease appears to hijack the normal aging process, research into prevention is prevalent. Smoking, obesity, and cardiovascular problems may be risk factors for the disease, so treatments for those may also help to prevent Alzheimer’s disease. Some studies have shown that people who remain intellectually active by playing games, reading, playing musical instruments, and being socially active in later life have a reduced risk of developing the disease.
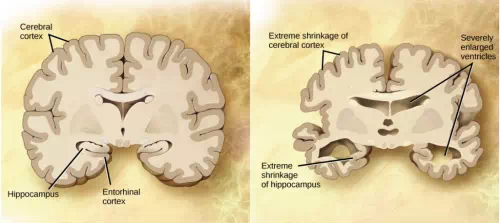
Figure 16.30. Compared to a normal brain (left), the brain from a patient with Alzheimer’s disease (right) shows a dramatic neurodegeneration, particularly within the ventricles and hippocampus. (credit: modification of work by “Garrando”/Wikimedia Commons based on original images by ADEAR: “Alzheimer’s Disease Education and Referral Center, a service of the National Institute on Aging”)
Parkinson’s Disease
Like Alzheimer’s disease, Parkinson’s disease is a neurodegenerative disease. It was first characterized by James Parkinson in 1817. Each year, 50,000-60,000 people in the United States are diagnosed with the disease. Parkinson’s disease causes the loss of dopamine neurons in the substantia nigra, a midbrain structure that regulates movement. Loss of these neurons causes many symptoms including tremor (shaking of fingers or a limb), slowed movement, speech changes, balance and posture problems, and rigid muscles. The combination of these symptoms often causes a characteristic slow hunched shuffling walk, illustrated in Figure 16.31. Patients with Parkinson’s disease can also exhibit psychological symptoms, such as dementia or emotional problems.
Although some patients have a form of the disease known to be caused by a single mutation, for most patients the exact causes of Parkinson’s disease remain unknown: the disease likely results from a combination of genetic and environmental factors (similar to Alzheimer’s disease). Post-mortem analysis of brains from Parkinson’s patients shows the presence of Lewy bodies—abnormal protein clumps—in dopaminergic neurons. The prevalence of these Lewy bodies often correlates with the severity of the disease.
There is no cure for Parkinson’s disease, and treatment is focused on easing symptoms. One of the most commonly prescribed drugs for Parkinson’s is L-DOPA, which is a chemical that is converted into dopamine by neurons in the brain. This conversion increases the overall level of dopamine neurotransmission and can help compensate for the loss of dopaminergic neurons in the substantia nigra. Other drugs work by inhibiting the enzyme that breaks down dopamine.
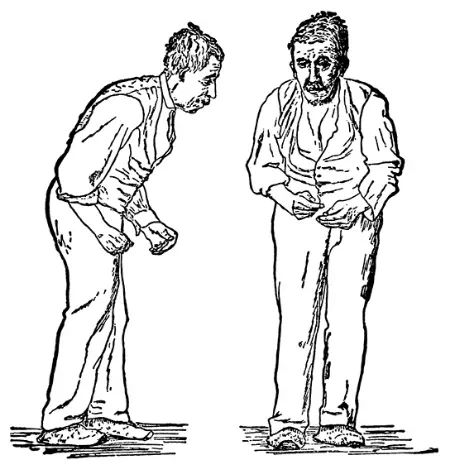
Figure 16.31. Parkinson’s patients often have a characteristic hunched walk.
Neurodevelopmental Disorders
Neurodevelopmental disorders occur when the development of the nervous system is disturbed. There are several different classes of neurodevelopmental disorders. Some, like Down Syndrome, cause intellectual deficits. Others specifically affect communication, learning, or the motor system. Some disorders like autism spectrum disorder and attention deficit/hyperactivity disorder have complex symptoms.
Autism
Autism spectrum disorder (ASD) is a neurodevelopmental disorder. Its severity differs from person to person. Estimates for the prevalence of the disorder have changed rapidly in the past few decades. Current estimates suggest that one in 88 children will develop the disorder. ASD is four times more prevalent in males than females.
A characteristic symptom of ASD is impaired social skills. Children with autism may have difficulty making and maintaining eye contact and reading social cues. They also may have problems feeling empathy for others. Other symptoms of ASD include repetitive motor behaviors (such as rocking back and forth), preoccupation with specific subjects, strict adherence to certain rituals, and unusual language use. Up to 30 percent of patients with ASD develop epilepsy, and patients with some forms of the disorder (like Fragile X) also have intellectual disability. Because it is a spectrum disorder, other ASD patients are very functional and have good-to-excellent language skills. Many of these patients do not feel that they suffer from a disorder and instead think that their brains just process information differently.
Except for some well-characterized, clearly genetic forms of autism (like Fragile X and Rett’s Syndrome), the causes of ASD are largely unknown. Variants of several genes correlate with the presence of ASD, but for any given patient, many different mutations in different genes may be required for the disease to develop. At a general level, ASD is thought to be a disease of “incorrect” wiring. Accordingly, brains of some ASD patients lack the same level of synaptic pruning that occurs in non-affected people. In the 1990s, a research paper linked autism to a common vaccine given to children. This paper was retracted when it was discovered that the author falsified data, and follow-up studies showed no connection between vaccines and autism.
Treatment for autism usually combines behavioral therapies and interventions, along with medications to treat other disorders common to people with autism (depression, anxiety, obsessive compulsive disorder). Although early interventions can help mitigate the effects of the disease, there is currently no cure for ASD.
Attention Deficit Hyperactivity Disorder (ADHD)
Approximately three to five percent of children and adults are affected by attention deficit/hyperactivity disorder (ADHD). Like ASD, ADHD is more prevalent in males than females. Symptoms of the disorder include inattention (lack of focus), executive functioning difficulties, impulsivity, and hyperactivity beyond what is characteristic of the normal developmental stage. Some patients do not have the hyperactive component of symptoms and are diagnosed with a subtype of ADHD: attention deficit disorder (ADD). Many people with ADHD also show comorbitity, in that they develop secondary disorders in addition to ADHD. Examples include depression or obsessive compulsive disorder (OCD). Figure 16.32 provides some statistics concerning comorbidity with ADHD.
The cause of ADHD is unknown, although research points to a delay and dysfunction in the development of the prefrontal cortex and disturbances in neurotransmission. According to studies of twins, the disorder has a strong genetic component. There are several candidate genes that may contribute to the disorder, but no definitive links have been discovered. Environmental factors, including exposure to certain pesticides, may also contribute to the development of ADHD in some patients. Treatment for ADHD often involves behavioral therapies and the prescription of stimulant medications, which paradoxically cause a calming effect in these patients.

Figure 16.32. Many people with ADHD have one or more other neurological disorders. (credit “chart design and illustration”: modification of work by Leigh Coriale; credit “data”: Drs. Biederman and Faraone, Massachusetts General Hospital).
Neurologist
Neurologists are physicians who specialize in disorders of the nervous system. They diagnose and treat disorders such as epilepsy, stroke, dementia, nervous system injuries, Parkinson’s disease, sleep disorders, and multiple sclerosis. Neurologists are medical doctors who have attended college, medical school, and completed three to four years of neurology residency.
When examining a new patient, a neurologist takes a full medical history and performs a complete physical exam. The physical exam contains specific tasks that are used to determine what areas of the brain, spinal cord, or peripheral nervous system may be damaged. For example, to check whether the hypoglossal nerve is functioning correctly, the neurologist will ask the patient to move his or her tongue in different ways. If the patient does not have full control over tongue movements, then the hypoglossal nerve may be damaged or there may be a lesion in the brainstem where the cell bodies of these neurons reside (or there could be damage to the tongue muscle itself).
Neurologists have other tools besides a physical exam they can use to diagnose particular problems in the nervous system. If the patient has had a seizure, for example, the neurologist can use electroencephalography (EEG), which involves taping electrodes to the scalp to record brain activity, to try to determine which brain regions are involved in the seizure. In suspected stroke patients, a neurologist can use a computerized tomography (CT) scan, which is a type of X-ray, to look for bleeding in the brain or a possible brain tumor. To treat patients with neurological problems, neurologists can prescribe medications or refer the patient to a neurosurgeon for surgery.